
The 2026 Medicare Physician Fee Schedule created an unusual situation for dermatology. On the surface, the headline looked positive. CMS finalized an increase to the Medicare conversion factor, a shift that many physicians welcomed after years of downward pressure. But as practices began reviewing the specialty impact tables and code-level changes, a more complex picture emerged.
For dermatology, the reality sits somewhere between optimism and caution. While the conversion factor increased for 2026, dermatology practices should not assume that translates into higher reimbursement overall. Specialty-level projections suggest that RVU redistribution and practice expense adjustments may offset conversion factor gains for certain procedure-driven practices.
This is not a contradiction. It is the nature of how Medicare payment is structured.
Dermatology, as a specialty driven by procedures, supplies, and practice expense inputs, is especially sensitive to redistribution effects within the Physician Fee Schedule. That makes 2026 a year where careful monitoring, financial modeling, and strong billing oversight matter more than usual.
Why Dermatology Is More Sensitive to Medicare Payment Shifts Than Many Specialties
Dermatology operates under a different economic model than many cognitive specialties. A significant portion of revenue comes from procedures performed in the office setting, many of which rely heavily on practice expense RVUs, supplies, equipment, and clinical staff support.
This structure makes dermatology particularly sensitive to RVU redistribution and cost assumption changes within the Medicare Physician Fee Schedule.
Specialties that rely primarily on evaluation and management services often experience slower, more gradual payment shifts. Dermatology, by contrast, can feel changes more quickly because so many services are tied to direct cost inputs and procedural valuations.
When CMS adjusts how it values staff time, equipment usage, or supply costs, those adjustments flow directly into the financial structure of dermatology practices.
This is why even modest policy changes can have a noticeable impact over time.
Why a Higher Conversion Factor Does Not Guarantee Higher Dermatology Reimbursement
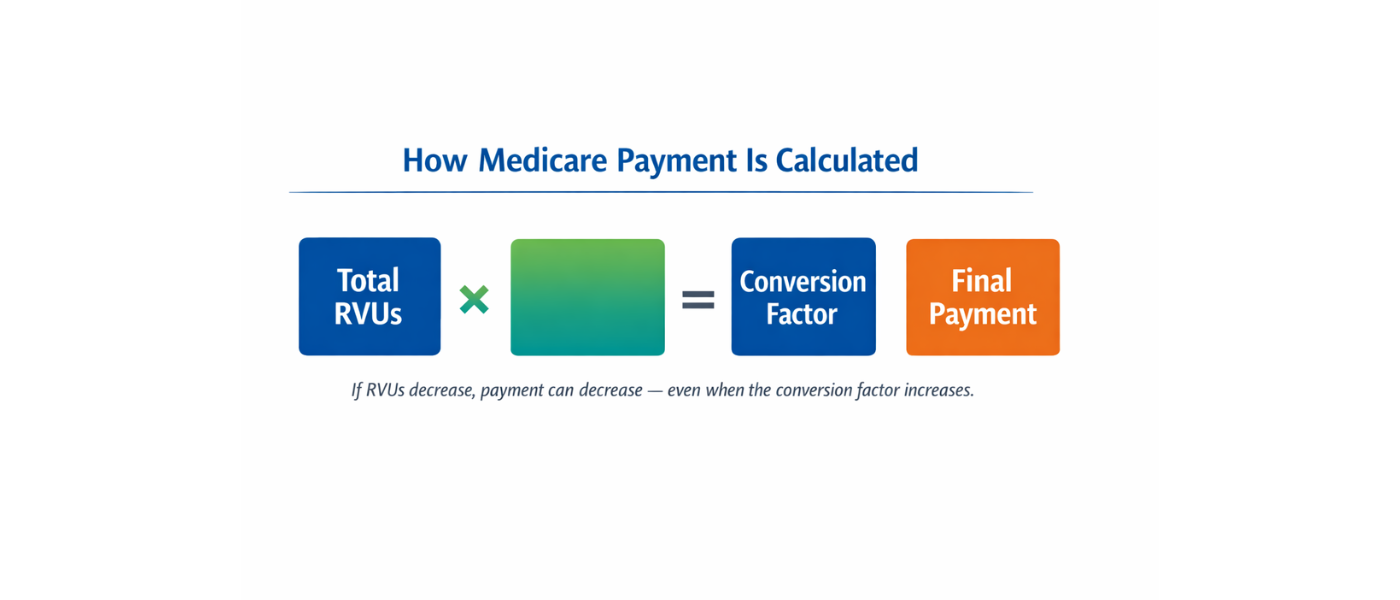
The conversion factor is only one component of Medicare payment. Final reimbursement is calculated by multiplying total RVUs by the conversion factor. When RVUs shift, practice expense inputs change, or efficiency adjustments are applied, the final payment can move in either direction regardless of what happens to the conversion factor itself.
For dermatology, the key pressure points in 2026 come from:
- Practice expense RVU redistribution
Direct cost input adjustments - Efficiency assumptions built into the payment model
- Site-of-service valuation differences
- Supply-driven procedure economics
Even small changes in practice expense allocation can have noticeable effects on dermatology because so many services rely heavily on equipment, supplies, and clinical staff time.
Although CMS finalized a conversion factor increase, statutory adjustments and RVU redistribution can still result in projected decreases at the specialty level. For dermatology, early specialty impact tables suggest that total allowed charges may not increase proportionally to the conversion factor. This reinforces the importance of analyzing reimbursement at the CPT code level rather than relying solely on the headline conversion factor percentage.
How the 2026 Medicare Changes Will Affect Dermatology Practices
The impact of the 2026 update is not uniform across dermatology. Two practices in the same city may experience very different financial outcomes depending on how their revenue is generated.
Medical dermatology practices with a strong evaluation and management foundation tend to see more stability. E/M services historically fluctuate less than procedural services, and practices that lean heavily into chronic disease management, acne, psoriasis, and dermatitis visits are less exposed to sudden shifts.
Procedure-heavy dermatology practices face more variability. Services such as:
- Biopsies
- Destruction of lesions
- Excisions
- Repairs
- Cryotherapy
- High-volume surgical procedures
are closely tied to practice expense RVUs. When CMS adjusts direct cost inputs or reallocates practice expense across specialties, these codes can see subtle but meaningful changes.
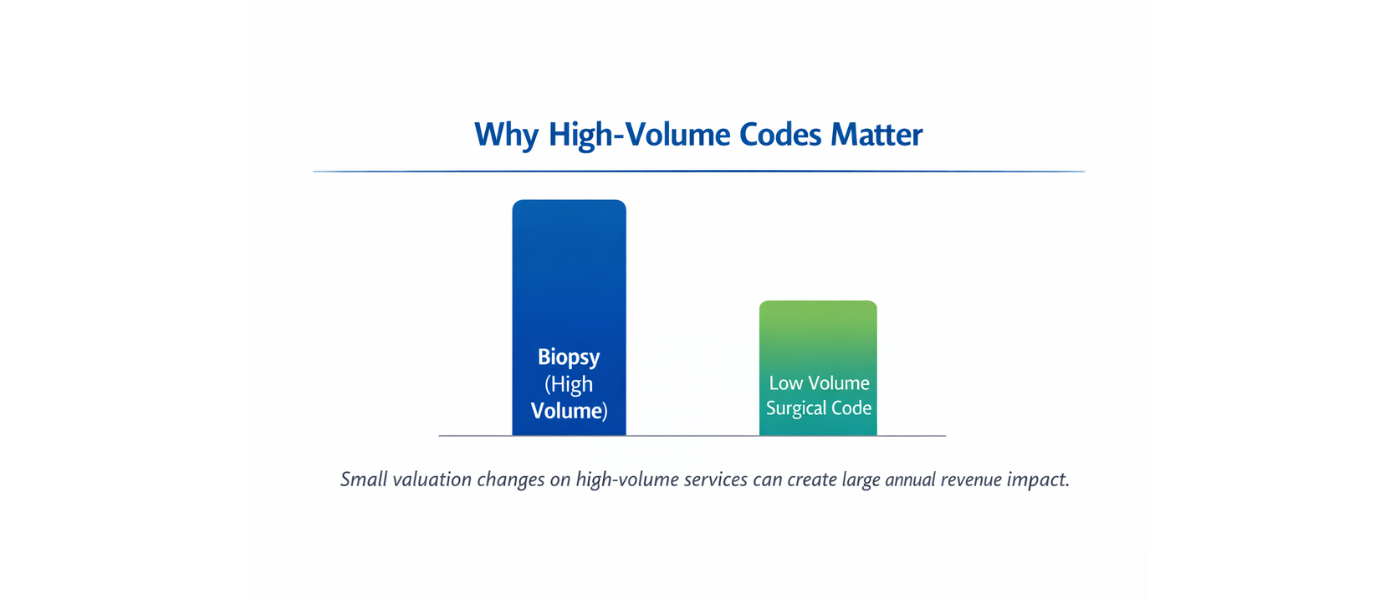
Even a small change applied across high-volume services can create measurable revenue impact.
For example:
A practice performing thousands of biopsies annually may not notice a small per-procedure adjustment at first glance. But over the course of a year, those incremental changes can add up to a meaningful shift in total collections.
This is why looking only at the conversion factor number can be misleading. Dermatology reimbursement is driven by volume, mix, and operational efficiency.
Facility vs Non-Facility Settings Matter More Than Many Realize
One of the more overlooked areas of the 2026 update is the difference in impact between facility and non-facility services.
Office-based dermatology relies heavily on non-facility payment structures. These payments incorporate practice expense components that reflect the cost of running a clinical environment. Changes to those cost assumptions affect dermatology more than specialties that perform services primarily in hospital settings.
Dermatology procedures performed in office settings may experience different financial pressure compared to those performed in outpatient facilities, where the practice expense component is structured differently.
This makes it especially important for dermatology practices to understand:
- Where their services are being delivered
- Which CPT codes drive the most revenue
- How site-of-service affects reimbursement patterns
Practices that track this data closely will be in a much stronger position to adapt.
How Practice Expense RVUs Shape Dermatology Reimbursement
Practice expense is one of the most influential components for dermatology reimbursement. Dermatology uses specialized equipment, supplies, and staff support for a large portion of its services. When CMS updates cost assumptions, supply pricing, or time allocations, those changes flow directly into RVU calculations.
Dermatology is particularly sensitive to:
- Supply-intensive procedures
- Equipment-dependent services
- Staff-supported treatments
- Repetitive high-volume services
These are exactly the areas where small RVU adjustments can have a ripple effect. It is also why dermatology practices often feel payment changes more quickly than cognitive specialties.
Mohs and Surgical Dermatology May Feel Changes Differently
Not all procedural dermatology is affected in the same way.
Mohs-heavy practices, for example, often operate with a different cost structure than general dermatology clinics. The combination of pathology, surgical time, clinical staffing, and equipment usage creates a layered practice expense profile.
When CMS updates practice expense assumptions, even small adjustments can influence:
- Stage-based procedures
- Repairs following excisions
- Staff time allocations
- Supply utilization assumptions
Over time, these changes can alter the margin on services that have historically been stable.
This does not mean Mohs practices are at a disadvantage. But it does mean they benefit from closely tracking reimbursement trends at the code level, especially when volume is high.
Medical Dermatology May See More Stability — But Not Immunity
Practices that lean heavily into medical dermatology often experience less volatility than procedure-driven clinics. Evaluation and management services tend to move more gradually than procedural valuations.
However, stability does not mean insulation.
Chronic condition management, biologic therapy monitoring, and high-frequency patient visits still rely on accurate documentation, correct coding levels, and efficient workflows. Even small shifts in documentation patterns or coding consistency can affect reimbursement outcomes when applied across large patient populations.
In years where procedure payments tighten slightly, strong E/M performance often becomes an important stabilizing force.
The Supply Cost Factor in Dermatology Economics
Dermatology is one of the more supply-intensive specialties in office-based medicine. Cryotherapy materials, biopsy tools, pathology-related supplies, surgical packs, anesthetics, and disposable equipment all contribute to the real-world cost of care.
When CMS updates supply pricing assumptions or practice expense allocations, those changes can subtly shift the valuation of services tied to those inputs.
Over time, supply-heavy procedures can feel these adjustments more than expected.
Practices that maintain strong internal cost awareness tend to adapt more effectively, especially when evaluating which services drive the greatest operational expense relative to reimbursement.
Why High-Volume Codes Deserve Close Monitoring
Dermatology tends to rely on a predictable set of high-volume CPT codes. When those codes experience even minor valuation changes, the impact multiplies quickly.
This is why practices should identify:
- Top 10 CPT codes by volume
- Top 10 CPT codes by revenue
- Codes with strong practice expense components
Understanding where the practice is most financially exposed is one of the most effective ways to stay ahead of Medicare changes.
This is also where strong billing data becomes a strategic tool rather than just an administrative function.
Documentation Accuracy Matters More in Tight Payment Years
When reimbursement pressure increases, accuracy becomes more important than ever. Practices should pay close attention to:
- Modifier usage
- Documentation completeness
- Code selection consistency
- Medical necessity support
In years when RVUs shift, even small documentation gaps can result in lost revenue, denials, or undercoding. A stable internal billing structure helps offset external reimbursement pressure.
What Dermatology Practices Should Do Now to Protect Revenue
The practices that navigate Medicare changes most successfully tend to be the ones that take a proactive approach.
Key steps include:
- Reviewing top CPT codes by utilization
Small valuation changes on high-volume services can quietly influence annual revenue. - Watching first-quarter EOB patterns
The January to March window often reveals how changes are actually being applied by payers. - Re-evaluating payer contracts
Commercial payers frequently align with Medicare trends. When Medicare shifts, contracts may effectively shift as well. - Running revenue projections
Understanding how different utilization patterns affect reimbursement allows practices to make smarter operational decisions.
Why 2026 Requires a More Strategic Approach for Dermatology
The 2026 Medicare update is not a crisis year for dermatology, but it is a year that reinforces how dependent the specialty is on RVU structure and practice expense economics.
The conversion factor increase provides some relief. But it does not fully insulate dermatology from redistribution effects within the Physician Fee Schedule.
Practices that understand their data, monitor their high-volume services, and maintain strong billing oversight will be in the best position to adapt.
The most important takeaway is simple.
No single number tells the whole story.
Dermatology reimbursement is shaped by procedure mix, documentation accuracy, practice expense inputs, and operational efficiency. The practices that pay attention to those details will continue to perform well even when Medicare payment models shift.